PFAS Are in Almost Everyone's Blood. Here's the Case That They're Killing People.
If you read this and it gets you worried about PFAS, two things you can do:
- If you are in a profession or place that has confirmed high levels of PFAS, consider signing up for the pilot of NeutraOat, a modified oat fiber that’s designed to remove PFAS from the gut and the blood. If you qualify, you’ll get 12 weeks of NeutraOat, plus before and after PFAS tests and blood panels. More info at the link.
- If you aren’t a firefighter or living in a contaminated place, consider reserving a spot in the first commercial batch of NeutraOat, coming out this fall. It requires a $20 refundable deposit, which helps us fund our first batch and prove to our investors that there’s commercial demand for this.
Each year, I estimate that somewhere around 3,400 heart disease deaths in the US are caused by PFAS, or forever chemicals, which raise cholesterol. PFAS also cause an additional 12,000 non-fatal heart attacks. If we put that in terms of QALYs (quality adjusted life years), which means we try to count how many years of life are lost and the quality of the remaining years, we find that about 50,000 QALYs are lost each year due to PFAS-caused heart disease, which is almost 10% of the QALYs gained by the use of statins.

Depending on where you sit on the political spectrum, this number may seem suspiciously low or high. And depending on how much you know about PFAS, cardiovascular disease may seem a weird health metric to focus on, given that PFAS have also been convincingly linked to cancer and immunodeficiency.
I’ll address the first concern, the exact quantification, later. For the second, I’ll just say that I wanted to focus on cardiovascular disease because there’s a lot of fear, uncertainty, and doubt around PFAS. The media has thoroughly confused PFAS with microplastics, and the steady parade of sensationalist microplastics claims (e.g. “there’s a credit card’s worth of microplastics in your testicles and brain”) followed by retractions (“actually we didn’t do a great job of avoiding contamination from lab gloves”) has cast a cloud of confusion over the popular understanding of PFAS as well.
But PFAS are not microplastics. The science is much more settled on what they are, and if (and how) they cause harm. Their extreme prevalence is also much better established, given how much easier they are to detect in blood than microplastics are. So we can take the most quantitative of the settled harm pathways, cholesterol-raising even at low doses, plus the settled prevalence, and come to a conclusion:
PFAS can and do kill people. The fact that they’re present in more than 95% of people, and that they have negative health effects at all doses, including very low ones, means they are almost certainly shortening your life expectancy as you read this.
But I understand most readers will want more than an assertion. People are rightly skeptical of environmental-toxin claims, especially in the liberal scientific world, and especially now that MAHA has poisoned the well. I could point to the lived experience of people I’ve met who’ve been personally damaged by PFAS:
 The Massachusetts city councilor who lost half a lung
The Massachusetts city councilor who lost half a lung
 The Michigan psychologist who lost a husband
The Michigan psychologist who lost a husband
 The Texas rancher who lost 85 cows
The Texas rancher who lost 85 cows
But the plural of anecdote is not data.
So instead I want to build the case for the harm of PFAS pillar by pillar, through a sort of Koch’s postulates of environmental contamination. I’ll argue for the danger of PFAS with:
- A specific molecular mechanism
- Animal models
- Human epidemiological studies
- And, finally, adversarial collaborations (lawsuits)

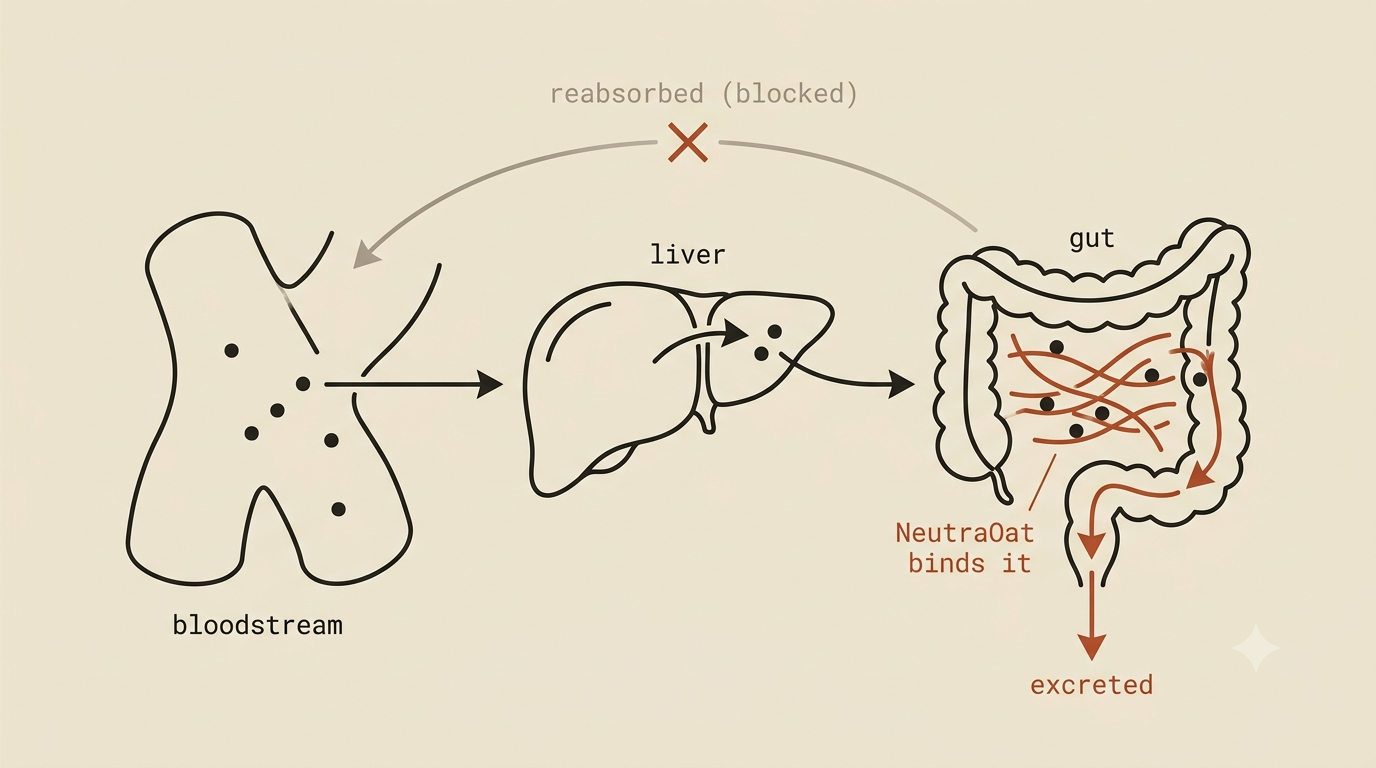
Before I begin: I’m not impartial here. I’m developing NeutraOat, a modified oat fiber designed to remove PFAS from the gut and bloodstream by interrupting the enterohepatic recirculation of small hydrophobic toxins. (When toxins cycle back into the gut from the bloodstream, NeutraOat is designed to pick them up before they can cycle back into the bloodstream again.) We’re running a human pilot in highly exposed people now, with first readouts in October.
I’m developing NeutraOat because I think PFAS is an important health issue, though you could also argue I think PFAS is an important health issue because I’m developing NeutraOat. Anyhow, with that disclaimer out of the way, onto the pillars.
We’re testing NeutraOat in highly exposed people now, with first results in October. If you want to be first in line at launch, you can reserve a place for a fully refundable $20.
Reserve my place →Pillar 1
PFAS has a clear molecular mechanism for harm
PFAS stands for per- and polyfluoroalkyl substances. If you remember any chemistry nomenclature, that tells you the core of what they are: many fluorines attached to the carbons of an alkyl chain. The carbon-fluorine bond is exceptionally strong and repels both water and oil. Some PFAS, including the oldest ones, like those used to make Teflon1, also have a charged head that’s attracted to water.
So what you get is a long, thin molecule that is very, very hard to break apart and may be attracted to water-loving surfaces. Unfortunately, that’s also how you’d describe a fatty acid, minus the “can’t be broken apart” part. Every transporter and target for fatty acids in the body therefore picks up PFAS, or gets hit by PFAS2, including albumin (the main fat-carrier in your blood) and PPAR-α (a master switch for fat metabolism and energy production).
This is also why PFAS end up “forever” in the body. Like fatty acids, they’re picked up and carried around by albumin. Unlike fatty acids, they aren’t broken down in the digestive tract or once they reach a target. If they’re in the digestive tract, they just get picked up and transported around again, only rarely getting excreted. If they’re activating a receptor, they just keep activating it.
So, on a molecular basis, PFAS are bad for you because they behave like fatty acids that can’t be broken down or digested. Basically anywhere a fatty acid can switch on a mechanism, PFAS can too, but they can’t be switched off.
Why this means there’s probably no safe dose
A natural question is how much your own PFAS level actually matters. You can look at cows suffering ataxia from insane levels of PFAS in their feed and see that’s obviously bad for the cows, while struggling to see why it matters at your own low exposure. In other words: does PFAS act on a threshold model, fine until a certain point and then not, or a linear model, where the danger gets worse with each additional molecule of PFAS in your blood?3
My answer is that PFAS is very much linear, and my excess-cardiovascular-death estimate depends on it. The theoretical case comes from Crump, Hoel, Langley, and Peto (1976). The short version: once a toxin plugs into a biological process that’s already running, its very first dose already buys some extra risk, which makes a genuine “safe threshold” hard to justify. (The full logic is in footnote 8, if you want it.)

The question that matters, then, is whether PFAS actually plugs into a process that’s already running. It does. Fatty acids are always in the body: they signal through PPAR-α, are carried by albumin and FABP1, and are cleared by renal OATs4. Thousands of times a day, a fatty acid gets carried by albumin to the liver, activates PPAR-α, then is degraded and cleared.
Every molecule of PFOA or PFOS in your serum runs the same pathways, but doesn’t get degraded. It keeps activating PPAR-α until something displaces it, so the target stays occupied longer than it should. However little that activation was going to raise your cholesterol5, it now raises it more. And since the log-linear link between serum LDL cholesterol and cardiovascular risk is one of the strongest findings in all of epidemiology, that’s clearly bad for you.
The only real escape hatch is a homeostatic mechanism that compensates, where, as PFAS push cholesterol up, fatty acids back off PPAR-α to bring it down, producing a threshold where cholesterol only rises once there are too many PFAS to compensate for. That’s a genuine possibility. But there are clues it doesn’t work that way. Even at relatively low PFOA (>4.9 ng/ml, which about half the population had in 20006), there still seems to be increased cardiovascular risk. We also see a steep rise in serum cholesterol at the very lowest PFAS doses in cross-sectional studies, though the HDL-vs-LDL relationship gets muddy in those same studies, and one can argue a steep low-dose rise is itself a sign of confounded causation7.
So on cholesterol alone, we get a reasonably strong push toward linear-no-threshold. Now the other quantitative effect: PFAS on vaccine response. Fair warning, this only adds a bit more push.
The molecular story for vaccine response is much muddier than for cholesterol, which is why I put it second. The basic shape is the same, in that fatty acids play a real role in vaccine response and PFAS play it too but can’t be degraded, but the specifics are far harder to pin down. Fatty acids seem to affect antibody differentiation and B-cell maturation through signalling, but a clean step-by-step story is as elusive here as anywhere in immunology, with all its redundancy and tangled causation. A linear argument would have to be that each extra molecule of indestructible PFAS messes up the signalling a little more.
The strongest empirical support for a linear vaccine effect is a series of studies on children in the Faroe Islands, which explicitly support a log-linear reduction in tetanus and diphtheria vaccine response even at very low PFOA. That sits uneasily with a German study that says a threshold model fits German children best, the study Europe based its PFAS limits on, which itself sits uneasily with a study arguing the German group did its stats wrong and should have fit a linear model (and which happens to be coauthored by the Faroe Islands researcher).
The underlying problem, if you haven’t picked it up: these studies are intensely political. They drive not just policy but the outcome of lawsuits, and “PFAS is fine below a threshold” vs. “PFAS is dangerous at low levels” is also a fight over how billions of dollars of cleanup gets spent.
For my money, I side with the Faroe Islands group, mostly because they point out the German study threw away an entire vaccine’s worth of data (Hib) for not being statistically significant at low levels. But very small effects at the lowest doses are exactly what you’d expect under a linear model. The first PFAS molecule should have a tiny effect, and if you discard everything below some effect size, you’ve forced yourself into a threshold model.
Pillar 2
PFAS kills animals, mice and bigger
A molecular mechanism is a nice story, but a story without evidence. Fortunately (or unfortunately), PFAS has the evidence.
At high doses, PFAS kills mice and rats, mostly through the liver but also wherever else fat ends up. They die of liver failure and cancer.
Of course, plenty of things kill rodents at high doses without being especially dangerous to us, like water or salt. Lab studies like these are unrealistic. So for a realistic path to harm, look at cases where large mammals were exposed to PFAS in the wild and died. There aren’t many, because the animals that get doses high enough for acute toxicity, namely pigs and cattle eating contaminated feed, are generally euthanized before they get the chance to die.
But there are some. The most shocking are in Texas, where “biosolids” (treated human sewage) were used as fertilizer around ranches. The waste was never tested for PFAS, and the treatment method actually concentrated it. So the cattle ate grass and drank water contaminated with highly concentrated PFAS.
In practice that looked like calves born with massive, fatal liver toxicity at a PFOS serum level of 610,000 ppt, 54 cows developing sudden ataxia and toppling over, and horses dropping dead. It also looked like the ranchers themselves developing thyroid cancer and diabetes.
Biosolids contain a lot of nasty chemicals, so we can’t pin all of that on PFAS. But it’s suspicious that the calf died of liver toxicity, at an enormous PFAS serum level, in exactly the way mouse fetuses die when their mothers get high PFAS doses. Combined with the mechanism from Pillar 1, the case starts to firm up.
Pillar 3
PFAS probably kills humans
Animals are one thing. Mice, cows, and horses die all the time. Humans dying is something we take more seriously.
Humans haven’t shown the dramatic acute toxicity that cows or mice have. We get relatively low doses over decades, which no animal study even tries to match, and it’s obviously unethical to dose people with high PFAS and watch. So we’re left with natural experiments: following the health of people who were exposed to high PFAS by accident. That’s more fraught than it sounds.
First, you need accurate health histories, and they don’t build themselves. Few health systems aggregate health data. Most of it sits with the doctor or the patient, and at best it’s aggregated for billing, usable for studies only with great care, given the incentives on both sides to inflate or deflate diagnoses.
Second, you have to isolate the effect of PFAS specifically. Many of the most exposed people, like factory workers or firefighters, are exposed to a whole stew of nasty chemicals. Firefighters especially inhale enormous quantities, so pinning down what caused a given cancer is hard.
Third, you have to trust the ground truth. You need the diagnoses to reflect diseases people actually have. That’s a real problem for something like thyroid cancer, which can be under-diagnosed (if nobody’s looking) or over-diagnosed (when they are, because many doctors will remove a thyroid on suspicion alone; once removed, “thyroid cancer” goes in the file with no confirmatory biopsy). Over-diagnosis is what led to huge numbers of Koreans getting thyroids removed with zero effect on actual mortality.
So I can point to suggestive studies showing PFAS might raise kidney and testicular cancer, but I’d rather not lean on those. I’d rather lean on the more boring, more robust findings: PFAS effects on immune response in children and on cholesterol. They hold up better against the three problems above:
- Accurate health histories: both immune response and cholesterol have been correlated with PFAS serum levels across many cohorts.
- Isolating PFAS: both the immune system and cholesterol use fatty acids as signalling molecules, so the Pillar 1 model predicts PFAS should affect both.
- Ground truth: cholesterol and vaccine titers are quantitative, more objective than a cancer diagnosis, and both have direct, well-established links to clinical outcomes.
PFAS likely has a wide range of effects in humans, but even sticking to just cholesterol and vaccine titers, we can directly impute deaths, in children and adults, to PFAS exposure. That’s how I got the cardiovascular estimate at the top (details in the methodology link).
Pillar 4
The health claims survived adversarial collaboration (court)
Most scientific claims are never really tested. A paper gets published; if others agree and want to build on it, they extend it; if they disagree, the options are narrower. You have to feel strongly enough to spend real time publicly disputing it, and far more often people just ignore it.
The PFAS health claims got tested, and not only in the literature. They were tested in court.
- DuPont was ordered to pay ~$670M over PFAS dumping that killed cows and probably caused cancer in people. That settlement funded the first big epidemiological study on PFAS, the C8 study.
- 3M was ordered to pay $10.3B for continuing to make PFAS products even after discovering (and hiding) that every blood bank in America was contaminated, and that high doses of PFOS can kill monkeys.
Both companies spent decades fighting their own employees who raised concerns about PFAS. When it came to court, they settled, despite having billions of reasons not to.
PFAS build up because they keep getting recycled through your gut. NeutraOat is a modified oat fiber designed to interrupt that loop, and we’re testing it in highly exposed people right now, with first results in October. If you want to be first in line at launch, reserve a place for a fully refundable $20.
Reserve my place →What this all means
Everyone’s heard the statistics: PFAS are found in the blood of 97% of Americans and last for decades. You’ve probably also seen the news. After the EPA finally set PFAS limits for drinking water in April 2024, it proposed in 2026 to rescind the limits for the newer, less-studied PFAS. PFAS is still a live issue in 2026, and depending on where you live, it may be in your drinking water.
That matters, and I don’t want to downplay it. You should be concerned about your water, especially well water that hasn’t gone through reverse osmosis. You should be concerned about your food, especially a lot of animal products from poorly regulated sources, since PFAS, like most contaminants, accumulates up the food chain.
But the bigger point is that I think PFAS is likely the most important environmental issue of our time. There are pollutants that are more widespread (carbon dioxide, maybe plastics), but none remotely as widespread and backed by such strong evidence of harm at low levels.
Put simply: everyone with any dose of PFAS is at some risk of PFAS toxicity. That’s 97% of Americans. The highest-dosed are at a lot of risk, and they have no way of knowing it unless testing has been done on their specific water supply.
That’s why I decided to work on PFAS. The science is real, and it’s killing people, including me.
What you can actually do
- Filter your water. There’s a lot of noise about which filters handle PFAS. My advice: get a reverse-osmosis filter and be done with it. If you’re on well water or your utility has flagged PFAS, this is the biggest single lever.
- Watch your food sources. PFAS accumulates up the food chain, so animal products from unregulated or contaminated sources are the higher-risk category.
- Find out where you stand. If you’ve lived near an airbase, a firefighting-foam site, or industrial contamination, or you’re a firefighter, a blood test tells you your actual exposure.
That covers what’s coming in. The harder problem is what’s already stored in you, because PFAS keep recirculating through that gut-to-blood loop for years. That loop is the problem I’m working on with NeutraOat: a modified oat fiber designed to bind hydrophobic compounds like PFAS in the gut and carry them out, so they can’t be reabsorbed and keep circulating. We’re running a human pilot in highly exposed people now, with first results in October 2026. I’m not going to tell you it works until my own data says so, but if you want to be first in line when it’s ready, you can reserve a place today.
The product
What NeutraOat actually is
If that worries you, here’s what I’m building about it. Three things make NeutraOat different from anything else you could take at home:
Selective by design
Activated charcoal grabs almost everything, nutrients and medications included. NeutraOat is oat fiber with water-repelling pockets designed to hold small contaminants like PFAS while passing over the larger structures that carry your vitamins. We’re still confirming how selective, so for now you space it a few hours from anything else you take.
Food-grade, no prescription
The closest thing that already exists is a prescription bile-acid drug that happens to bind PFAS, but it’s prescription-only and hard on your nutrients. NeutraOat is designed to be a gentler, food-grade take on the same idea, something you can actually keep in the cupboard.
Twice a day, before meals
It’s a mild oat-fiber powder: 4 g a day during the active phase, then 2 g a day to maintain. It mixes into water, yogurt, or oatmeal and tastes like plain oat fiber.
Why I think it works
The mechanism is established. Cholestyramine, a prescription bile-acid binder that works the same way in the gut, lowered PFOS by about 60% in a published 2024 trial. NeutraOat is designed to do the same job in food-grade form, at a lower dose, and to be more selective about what it binds.
I’m not going to tell you it works until my own data says so. A human pilot in highly exposed people is running right now, with first results in October 2026. Reserving holds your place for a product in active testing. It isn’t a treatment, and it isn’t a drug approved to treat or prevent any disease.
Be first in line.
NeutraOat will launch at $60 a bottle, about a month at the active dose plus two at maintenance. Reserve one now for a fully refundable $20 deposit, credited in full toward your first bottle. You get launch priority and the October pilot results before anyone else.
Reserve my place →Methodology
The full calculation behind the ~3,400 cardiovascular deaths and ~50,000 QALYs is in this document, kept open so you can check the work.
Footnotes & go deeper
- The oldest types of PFAS (the “long chain” PFAS) are also the best studied, specifically PFOA and PFOS. Most of my claims above are based on studies done on those specifically.
- This is most true for long-chain, legacy PFAS, and less true for short-chain, newer PFAS. It’s also why long-chain PFAS last longer: they’re better fits for albumin and so keep being transported. One of the big controversies in the field is whether the new short-chain PFAS are actually safer. The case for: they’re less similar to fatty acids and clear much faster (days to weeks vs. years). The case against: they likely cross barriers more easily, including gestational and organ barriers.
- The term “linear” here is a bit misleading. “Additive” is more accurate, since what matters is that risk goes up with each additional molecule, not the exact shape of the line.
- Organic anion transporter. Not, you know, oat fiber, like NeutraOat.
- This is oversimplifying. Fibrates are a class of drug that agonize the PPAR-α receptor, so they’re designed to do on purpose what I’m saying PFAS do by accident. They’ve historically been used to lower cholesterol, the opposite of what I’m attributing to PFAS. But in a subset of patients they raise LDL, and that gives them a mixed signal on cardiovascular endpoints, raising risk in some patients, which soured the field on them. Translating a temporary agonist tested in a high-cholesterol population to a permanent, indestructible agonist present in nearly everyone, I think we strengthen the conclusion that PFAS is bad for cholesterol.
- Caveat: now only ~2% of the US population has >4.9 ng/mL PFOA, because PFOA has been phased out in favor of newer-generation PFAS. Even as a “forever chemical,” PFOA still slowly clears over years. Does that turn this back into a threshold issue, or do the same conclusions apply to new PFAS? See footnote 2, we’re chasing a moving target.
- The argument: yes, high PFAS can cause high cholesterol. But PFAS and cholesterol recirculate via the same enterohepatic pathway (also foundational to how NeutraOat works), so anything affecting cholesterol clearance also affects PFAS clearance. Someone with high cholesterol clearance would also tend to have low serum PFAS, and vice versa. I’m not fully convinced this explains the curve shape better than dose response, but it does make interpretation more complicated.
- The formal version, from Crump, Hoel, Langley, and Peto (1976): there are two possibilities for a carcinogen. Either the first dose buys zero extra risk (a threshold model), or the first dose buys some extra risk (a linear model). If you take a biological process that’s already running and can cause disease, it can’t be in the first category, because there’s already some risk at some dose. So we already have some kind of linear model. The only remaining possibilities are that every prior dose added risk but we’ve hit a ceiling, so further doses add zero, or that we haven’t hit a ceiling. And if there were an acute ceiling, like sudden death, then any organism that isn’t dead hasn’t hit it yet.